 German
German Ελληνικά
ΕλληνικάThe superior oblique muscle is innervated by the fourth cranial nerve (trochlear) and its effect is to shift the eye downwardly and inwardly (nasally).
The superior oblique muscle is innervated by the fourth cranial nerve (trochlear) and its effect is to shift the eye downwardly and inwardly (nasally).
Frequently, a child may be born with partial or even complete paralysis of the superior oblique, either because of anatomical damage of the muscle itself, or due to a malfunction of the trochlear nerve.
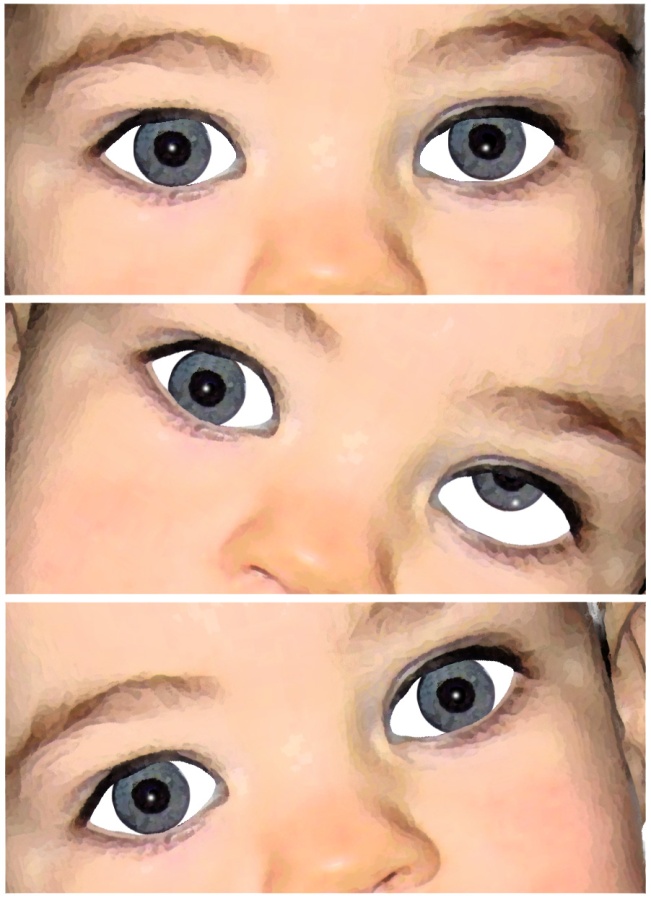 In paralysis of the superior oblique the upper corner of the eye is hardly noticeable when the child is looking straight ahead (primary eye position). We notice the maximum upper shift when the child turns his gaze the opposite side from the side of the paralysis and tilts his head towards the shoulder of the paralyzed muscle. But if he tilts his head towards the shoulder that is in the opposite side of the paralysis, then the eyes are aligned.
In paralysis of the superior oblique the upper corner of the eye is hardly noticeable when the child is looking straight ahead (primary eye position). We notice the maximum upper shift when the child turns his gaze the opposite side from the side of the paralysis and tilts his head towards the shoulder of the paralyzed muscle. But if he tilts his head towards the shoulder that is in the opposite side of the paralysis, then the eyes are aligned.
There is a characteristic counter-position that patients take with unilateral superior oblique palsy, by lowering the chin, turning and tilting the head towards the opposite side of the paralysis.
The treatment here is surgical.